Procedures, prevention and treatment of acute myocardial inarkt period of 2012-2014, the cardiology clinic in Skopje
Summary
INTRODUCTION: Acute myocardial infarction is an acute coronary ischemia leading to myocardial necrosis.This disease is widespread in the world and as such is still a hot topic for processing. The benefit of its wide distribution and the fact that heart diseases are still the leading cause of death worldwide. 40% to 50% of deaths are due to heart disease. Macedonian practice shows that heart disease is present in a high percentage. Up to 60% of all deaths are attributed to this kind of disease. Survival in developed countries today is 95%.
PURPOSE: reduction of the clinical problem, the pathophysiological mechanism (decline of tissue, atherosclerosis), reduction of the symptoms (pain, dyspnea), complications (sudden death, thromboembolism, arrhythmia, heart failure progression) or new cardiovascular event, reducing the dependence of other people, increased efficiency, increased self-esteem.
MATERIALS AND METHODS: research activity is made using a statistically data JZUU Cardiology Clinic for three years and 2012. 2013. and 2014.
RESULTS: showed that the number of patients with coronary disease or acute myocardial infarction in emergency reviewed clinic- grow, and inversely proportional to age.
DISCUSSION: In 2012, there were 16,138 inspections in emergency clinic, of which 616 patients with MI.In 2013 performed 17 177 examinations of which 846 patients with me.In 2014 performed 19 423 examinations of which 1124 patients with MI. The patient with acute coronary disease or AIM (Acute Coronary Syndromes) is a medical emergency and require coordinated and efficient service from all members of the multidisciplinary team, especially on the initial assessment and treatment of these patients. In recent years there has been a real improvement of services for patients with coronary disease. Challenges remain for maximizing infrastructures and forces between them in order to deliver the best possible care to all who would benefit. The main objective is to reduce morbidity and mortality, and improvement in life expectancy, which in the course of life will have reduced exposure to risk factors related to lifestyle.
Key words: Acute coronary syndromes, stroke, coronary disease
Sažetak
UVOD: Infarkt miokarda je najteži oblik akutne ishemijske bolesti srca. U procesu nastaje potpuno začepljenje koronarne arterije što dovodi do nekroze miokarda zbog nedostatka krvi i hranljivih materija bogatih kiseonikom.
CILJ: ovog rada je utvrditi procedure za definiranje akutnog infarkta miokarda, različite faktore uzroka, sprečavanje i podizanje svijesti o faktorima rizika kod svakog pojedinca i borbi za smanjenje ili eliminaciju faktora rizika koi će biti opisani,,mozni komplikacii i najvažnije pravovremena dijagnoza i pravovremeno liječenje i sprovodzenje terapije.
MATERIJALI I METODE: Za istražovanje su korišteni statistički podaci JZUU Klinike za kardiologiju. Istraživanje je provedeno u period od tri godine i to: a 2012. 2013. i 2014. godine.
REZULTATI: pokazuju da je broj pacijenata sa koronarnom bolesti ili akutnim infarktom miokarda u stalnom porastu.
DISKUSIJA: U 2012. godini, obavljeno je 16.138 hitnih pregleda, od kojih je 616 pacijenata sa infarktom miokarda. U 2013 obavljeno 17. 177 pregleda od kojih 846 pacijenata sa infarktom miokarda, dok je u 2014 obavljeno 19. 423 pregleda od kojih 1124 pacijenata sa infarktom miokarda. Pacijent sa akutnom koronarnom bolesti ili AIM (akutnim koronarnim sindromom) je hitan slučaj i zahtijeva koordiniranu i kvalitetnu uslugu od svih članova multidisciplinarnog tima, posebno kada je u pitanju inicijalna procjena i liječenje ovih bolesnika.
ZAKLJUČAK: Cilj je smanjiti morbiditet i mortalitet, omogućiti poboljšanje životnog vijeka, te uticati na smanjenje faktorima rizika koji utiču na kvalitet života.
KLJUČNE RIJEČI: akutni koronarni sindrom, stemi, moždani udar, koronarna bolest.
Introduction
Acute myocardial infarction is an acute coronary ischemia which leads to necrosis. MI- myocardial infection could be explained as a death of cells in heart muscle (myocardium) extension caused by ischemia. MI results with complete blockage of the coronary arteries. The infected region and the myocardium itself are becoming necrotic and non-functional. Although cardiac chambers are filled with blood the heart’s blood supply is completely controlled by the coronary arteries. So if they are non-functional, the entire blood supply of the heart would be violated.
The myocardial infection is still extremely presented disease in the world and remains one of the most discussed topics in the medicine. Leading cause of death in the world are heart diseases, responsible for 40% to 50% of overall death cases. Macedonia is not an exception, namely Macedonian practice shows that heart diseases among the Macedonian population are present in a high percentage. Up to 60% of all deaths are caused by heart diseases. However, survival percentage in developed countries today is pretty high, approximately 95%. Reduced clinical problems, pathophysiological mechanism (tissue lose, atherosclerosis), softer symptoms (pain, dyspnea), reduced complications (sudden death, thromboembolic disease, arrhythmias, heart failure progression) and prevention from new cardiovascular infarct, are decreasing dependence of other people, increasing efficiency, and better in high percentage the psychological health of the patients.
Coronary arteries can gradually narrow from lipid deposits, which will be converted into atherom plaque below the intimacy that covers the blood vessels. The Intima can perforate, and plaque becomes exposed to the blood flow in the artery. This immediately initiates the formation of thrombus. Blood vessels are plot of plaque, it becomes okluditan because of thrombotic. Currently, the infected region of the chamber, responsible for blood supply, becomes necrotic. Chambers’ focus is on the hypoxic region around infarct and they become very irritable, which may cause fatal arrhythmias1.
Acute myocardial infarction is determined by the criteria of the classical ischemia and has the same symptoms, chest pain, evolutionary changes in the ECG, which includes the development of Q-waves, an increase in creatine kinase to two times higher than the upper reference limit. At least two of these criteria must still be met in order to be diagnosed acute MI. Clinical division has been made, which divided them into two groups: STEMI and NON -NSTEMI. STEMI is characterized by ST segment elevation, while NON-STEMI is characterized by not increase3 (Picture 2).
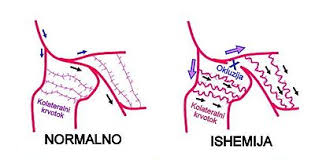
Picture 1: Normal case vs. Ischemia
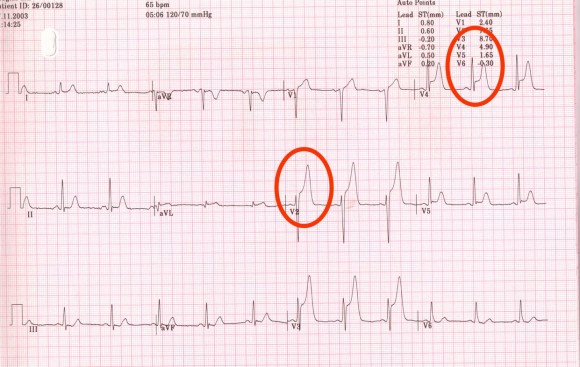
Picture 2: Stemi
Source: Hypoxia induces first reversible and in the final stadium irreversible necrosis of the muscle tissue, which could result with heart failure, arrhythmias, stroke, or sudden death. Rare cause could be also cramp embolism, aortic or post manipulation2.
Symptoms
- Extremely strong pain
presternal, radiation-left arm or both arms, neck, mandible, coat of arms, epigastric, abdominal-rare.
- Fear of death
- Paleness
- Sweating
- Dyspnea (less often with cyanosis)
- Hypo- or Hypertension
- Tachycardia (bradycardia less frequently)
- Bradycardia
- Gallop rhythm
- Signs of heart failure
- Interrupt latency
- Lungs changes
- Hypotension
- Shock.
There are cases of acute myocardial infarction, which are characterized by no pain. Common reasons for such cases are diabetes, neuropathy, alcoholism, age, heart transplant.
Complications
- Tachyarrhythmias
- extra systolic
- Ventricular tachycardia or fibrillation (clinical death)
- Atrial fibrillation,
- Bradycardia-three degrees AB block (block Total is with extreme bradycardia with heart rate lower than 30 otčukuvanja in minutes and the risk of death)
Possible complications are also acute heart failure in pulmonary edema or shock.
Another complication that can occur is the valves rupture, on the septum or on the heart chords, which could be fatal for the patient.
Other possible complications are immunological Pericarditis (Dressler sy.), Thromboembolic on the CNS or the lung, as well as sudden cardiac death4.
Myocardial infarction implies total occlusion of the coronary arteries that can be diagnosed with EKG. The electrocardiogram will also show us which of the coronary arteries (or branches of the coronary arteries) are blocked and is also able to detect blocks in the heart chambers caused by the infarct8.
ECG with ST elevation (STEMI), ECG without ST elevation (NON-STEMI), or less common but also possible, EKG with ST depreciation is the first sign of myocardial infection. Another signs that imply the presence of the MI and could be detected on the ECG are the negative T-wave and the Q wave, which is actually necrosis that could be also consequence of some previous MI. Biochemical markers are tropinin and tropinin T (cardiac enzyme) and CPK and CPK-MB36.
Therapy
The knowledge gained in the recent years helped in the creation of more protocols for medical therapy. The medical therapy can be either invasive or non-invasive.
The goal of therapy is to prevent the adherence of developed tubers on the broken plaques, which will prohibit the process of healing and strengthening of the plaques, which eventually should prevent and avoid future ischemia7.
Treatment should be as fast as possible (in the first 30 minutes of the onset of symptoms), to reduce the level of heart damage. When the treatment is prolonged the heart damages could be much more greater and the positive outcome of the treatment is highly uncertain5.
Figure 1. Graphical representation of the increase in patients with MI per year
Source:
The nurse’s task
Most essential for the nurse is to recognize all of the discussed medical conditions in order to be able to treat them and help the patient. All important decisions are made by the medical doctors, but in some certain nurse’s urgent intervention is crucial. Quick response of the medical doctor and his/her instructions are substantial for the nurse’s intervention and the nurse should wait on them to start the care for the patient11.
Most of the death cases are noted at the beginning of the myocardial necrosis, as a result of ventricular fibrillation. In such a cases a proper medical help should be given as quick as possible in order to achieve maximum effect of it, which first of all should include defibrillation and reperfusion. If ventricular fibrillation develops professional medical help should be given in the early stages of the condition. The successful resuscitation is crucial for survival of the patient. When transporting the patient it should be known that he/she in non-case should be the driver, but to immediately call emergency that will transport the patient appropriately to the hospital12.
Purpose of treatment
- Elimination of the clinical problems, the pathophysiological mechanism (decline of tissue, atherosclerosis)9
- Softening the common symptoms such as pain in the chest and dyspnea
- Preventing the complications which could be sudden death, thromboembolism, arrhythmia, heart failure progression
- Eliminating the possibility of new cardiovascular event
- Reducing the dependence of other people
- Improving the self-esteem of the patient
- Increasing the efficiency of the whole procedure
Materials and methods
The research activity is conducted on actual statistical data gained from the “JZUU Clinic of Cardiology” Skopje, Macedonia in time period of three years 2012, 2013 and 2014.
Results
The results from the research have shown that the group of patients with coronary disease or acute myocardial infection is extremely fast-growing group, accordingly to patient’s age. Namely, the probability to develop coronary disease or myocardial infection increases with the patient’s age.
Total 2189 patients were analyzed in the period of from 2012 to 2014 years. In this period, the reported 1890 patients hospitalized patients 299, hope for tertiary health care (PHI University Clinic for Cardiology and other clinic in Skopje). During the analyzed three years in the Clinic for Cardiology-Skopje-2012th 2012 2013 2014 total resided 2,189 patients of whom 1,523 patients of male gender, 666 patients of the female sex. In Table 1 is represented representation of patients by half for each year 16%). From the study, it is concluded that each year is increasing the number of patients who are the reported and hospitalized in the Clinic for Cardiology-Skopje
Table 1. Analysis of the patients and the number ratio
| pole | 2012 | 2013 | 2014 | total |
| Male | 408 (71,8%) | 476 (63,7) | 639 (73,1%) | 1523 (69,6%) |
| female | 160 (28.2%) | 271 (36.3.%) | 235 (26.9%) | 666 (30.4%) |
| total | 568 | 747 | 874 | 2189 |
Table 2. Analysis of the patients and the number ratio
Table 3. Analysis of the patients by age
| Grups age | total | |||
| tо 45 | 57(10%) | 69(9,2%) | 86,(9,8%) | 212(9,7%) |
| 46-55 | 134(23,6%) | 161(21.5%) | 215 (24,6%) | 510(23.3%) |
| 55-60 | 197(34.7%) | 259(22.2%) | 277 (31.4%) | 733 (33.5%) |
| over 60-70 | 141(24,8%) | 177(23.7%) | 201(23.3%) | 522(23.8%) |
The analysis of the patients by age shows that the eyelid patients in all analyzed years are represented by the 55 th to the 60 th year about 733 (33.5%), a minimal number has what age group to 45 this year which reached 212 (9, 7%).
Table 4. Number and percentage of hospitalized patients of the total number of patients who stayed in Clinic for Cardiology-Skopje:
| 2012 | 2013 | 2014 | total | |
| Hospitalized | 22 | 89 | 188 | 299 |
Of the total number of patients who come forward for review hospitalized at the Clinic for Cardiology-Skopje:2012 -22 patients, 2013-89 and 2014-188 patients,total 299.
Discussion
Clinical practice has shown that the number of patients with coronary disease or acute myocardial infarction is extremely fast growing. The statistical data confirms this claim. In year 2012 in the emergency center of the Clinic of Cardiology in Skopje, Macedonia were noticed 16,138 cases of patients with myocardial diseases, from which 616 patients were diagnosed with myocardial infarct. In year 2013 were archived 17,177 cases, from which 846 patients were diagnosed with myocardial infarct. In year 2014 were conducted 19,423 medial inspections from which 1,124 patients were again diagnosed with myocardial infarct. The analysis of the patients by age shows that the eyelid patients in all analyzed years are represented by the 55 th to the 60 th year about 733 (33.5%), a minimal number has what age group to 45 this year which reached 212 (9, 7%). Of the total number of patients who come forward for review hospitalized at the Clinic for Cardiology-Skopje:2012 -22 patients, 2013-89 and 2014-188 patients,total 299.
From all statistical data and clinical practice we surely conclude that heart diseases are still one leading causes for death in the world. Republic of Macedonia is not an exception, 60% of the deaths are induced from heart diseases. The death cases are 600 of 100,000 per year.
Conclusion
Patients with acute coronary disease or AMI (acute coronary infarction) are categorized as urgent patients and they require highly coordinated and high quality multidisciplinary medical team, especially in the initial assessment and treatment of these patients. In recent years real improvements of the medical service and medical treatment for patients with coronary artery disease have been made10. Optimizing the infrastructure in order to deliver the best possible care for all patients is still a challenge, but gradual improvements are being made. The main goal is to reduce mortality and increase life expectancy, that in the course of life will be reduced, primarily because of the exposure to risk factors related to lifestyle.
Literature
1.Flin, А. G. (2011) American Manual of Clinical Medicine
2.Hacked, R.Thompson, R. D. (2012) Nursing Care in Cardiology
3.Vorel, A, D.iKoks, M, T. IFIRT, D, G. (2012) The Oxford textbook of medicine 4.Balady, G. J., B. J. Fletcher, E. S. Froelicher, L. H. Hartley, R. M. Krauss, A. Oberman,
5.Blair, T., L. Morrin (2001): Resistance Training Guidelines, American Heart Association, American College of Sports Medicine, Canadian Association of Cardiatic rehabilitation
6.M. L. Pollock, C. B. Taylor, (1994): A Statement for Healthcare Professionals, American Heart Association
7.Findak, V., M. Mrakovič (1997): Pračenje i vrednovanje u tjelesnoj i zdravstvenoj kulturi, sportu i sportskoj rekreaciji. Napredak 138 (3); 315-317
8.Koturovič, Lj., S. Solarič, Z. Stanič (1979): Kineziterapija-tjelesno vjezbanje kao način i oblik prevencije, terapije i rehabilitacije, Sportnomedicinske objave, broj 10-12, Ljubljana
9.Fletcher, G. F.,G. Balady. V. F. Froelicher, L. H. Hrtley, W. L. Haskell, M. L. Pollock (1992): Exsercise Standards, A Statemant for Healthcare Professionals From the American Heart Association, American Hert Association 86; 340-342
10.Keber I. Ambulantna rehabilitacija u ranoj rekonvalescenciji poslije akutnog srčanog infarkta. U: Turkulin K. (urednik). Medicinska rehabilitacija i ocjena radne sposobnosti srčanih bolesnika. Krapinske Toplice, 1984: 205-208.
11.Turkulin K. Rehabilitacija i ocjena radne sposobnsoti srčanih bolesnika. U: Turkulin K. (urednik). Medicinska rehabilitacija i ocjena radne sposobnosti srčanih bolesnika. Krapinske Toplice, 1984: 145-154.
12.Клиниката за Кардиологија-Скопје и истории за болеста од пациентите и превенции..Флин, А. Г (2011) Американски прирачник за клиничка медицина